Is Your Child "Double-Jointed"? Understanding Hyperlaxity and Planovalgoid Feet
- Vaibhav Mittal
- 2 days ago
- 3 min read


Medically Reviewed By: Dr. Vaibhav Mittal, MS Orthopaedics (Paediatric Orthopaedic Surgeon)
Last Updated: June 2026
Many parents visit my clinic concerned because their child seems unusually flexible, often describing them as "double-jointed." Along with this extreme flexibility, parents frequently notice that when the child stands, their feet look completely flat, and their ankles seem to roll heavily inward.
In paediatric orthopaedics, we refer to this combination as Generalized Ligamentous Hyperlaxity paired with Planovalgoid Feet.
While these medical terms sound intimidating, the conditions themselves are incredibly common and, in the vast majority of cases, entirely harmless. Here is a clear guide to help you understand why your child’s joints move the way they do, how it affects their feet, and when it actually requires medical attention.
What is Hyperlaxity (Hypermobility)?
Ligaments are the strong, rubber-band-like bands of tissue that connect bones to other bones, keeping our joints stable. In some children, the collagen proteins that make up these ligaments are naturally stretchier than average.
This means their joints have a wider range of motion than typical. You might notice that your child can:
Bend their thumb all the way back to touch their forearm.
Hyperextend their elbows or knees backwards.
Place their palms completely flat on the floor without bending their knees.
For most children, this "benign hypermobility" is just a normal variation of human anatomy. It is often genetic—if you or your spouse were highly flexible as children, there is a good chance your child will be, too.
How Does Hyperlaxity Cause "Planovalgoid" Feet?
Because the ligaments in a hyperlax child are stretchier, they do not provide as much rigid support to the bones of the foot when the child stands up.
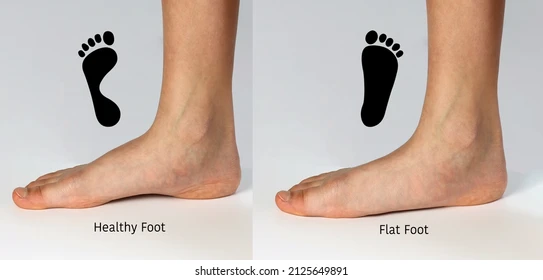
This leads to a specific posture called the Planovalgoid foot:
Plano (Flat): The stretchy ligaments allow the arch of the foot to collapse under the child's body weight, making the sole rest completely flat on the floor.
Valgoid (Valgus): Because the midfoot collapses, the heel bone tilts outward, causing the inner ankle to prominently roll inward toward the other leg.
When the child sits down or stands on their tiptoes, the arch usually magically reappears. This proves that the joints are flexible and healthy, not structurally deformed.
Will It Cause Long-Term Problems?
This is the number one worry parents have. The reassuring truth is that for a healthy, active child, hyperlaxity and planovalgoid feet are usually painless and do not cause long-term joint damage or arthritis.
In fact, extra flexibility can be an advantage in sports like gymnastics, swimming, or dance. Because the muscles have to work a little harder to stabilize the loose joints, children often naturally build the strength needed to support themselves as they grow.
When Should You Be Concerned? (The Red Flags)
While observation is the best treatment for painless hypermobility, you should schedule a clinical evaluation if your child experiences any of the following:
Frequent Joint Pain: Complaining of aching knees, ankles, or feet, especially after playing or at night.
Refusal to Walk: Asking to be carried frequently because their legs get tired much faster than other children their age.
Recurrent Sprains or Dislocations: Because the ligaments are loose, some children are more prone to rolling their ankles or experiencing joint subluxations (partial dislocations).
Clumsiness and Frequent Falls: Struggling with balance or constantly tripping over their own feet.
A "Rigid" Flat Foot: If the foot remains completely flat and stiff even when the child sits or goes on their tiptoes, it requires orthopaedic assessment.
How Do We Manage It?
If your child is diagnosed with symptomatic hyperlaxity and planovalgoid feet, our goal is to improve their stability and reduce fatigue.
Watchful Waiting: If there is no pain, we simply monitor their development. Aggressive treatment is unnecessary for painless flexible flat feet.
Physical Therapy: This is the most effective intervention. We teach targeted strengthening exercises for the core, hips, and lower legs. Stronger muscles act like internal braces, compensating for the loose ligaments and holding the joints in better alignment.
Supportive Footwear: For children with pain or extreme fatigue, we may recommend shoes with a firm heel counter (the back of the shoe) to stop the ankle from rolling inward.
Custom Orthotics: We rarely use rigid plastic inserts anymore. However, in cases of severe foot fatigue, a soft, custom-molded arch support can temporarily help position the foot correctly and relieve stress on the inner ankle.
Surgery: Surgical intervention for flexible planovalgoid feet is exceptionally rare and is only ever considered for older teenagers with severe, debilitating pain that does not respond to years of conservative treatment.
A Note to Parents: Do not rush out to buy expensive, rigid orthopedic shoes just because your toddler has flat feet. Let them play barefoot on soft, uneven surfaces like grass or sand as much as possible. This forces the tiny muscles in their feet to constantly fire and balance, which is the best natural therapy for building a strong arch.


Best pediatric orthopedic doctor ,well behaviour and good facilities Dr Vaibhav Mittal is best surgeon